COVID-19: Truth, Conspiracy, or SNAFU—YOU Decide.
The FULL MONTY!
Will COVID-19 kill you?
Will the economy re-open?
by L. Reichard White
[email protected]
![]()
Attribute to L. Neil Smith’s The Libertarian Enterprise
We will not escape from this misery until the
Government has been forced to admit that it made a foolish mistake and
over-reacted wildly to Covid-19.
—The BBC's Peter Hitchens
A snowball's chance in the hot place comes to mind. Rather than waiting for that ice water, as usual, we'll have to straighten this out for ourselves.
So, do you believe COVID-19 will kill you? And will the economy re-open? The two answers are joined at the hip.
Because it's not so much the virus that needs to be brought under control, it's the establishment narrative, fake news and urban myth about the virus.
That is, as you'll see, it's not the virus pandemic we have to worry about, it's the Narrative Pandemic .
Let's get that truth nailed-down right now .
First the context we get from this: " C.D.C. estimates 24,000 to 62,000 U.S. flu deaths occurred [in the ~six months] from Oct 1, 2019 thru March 21, 2020. "
An estimate when the actual data exists? What would it be for a full year? And with a range of 38,000, it's clear they didn't bother to actually do a tally. Why don't they keep their numbers up-to-the-minute? So where did their numbers come from?
They use computer simulations—but why use simulations instead of tallying data that already exists? What about the COVID-19 numbers they're feeding us?
Indeed, all the constantly changing scare projections are done with computer simulations appropriately called "models" which must always be based on programming assumptions . That's why some nerds call them " technical fiction ."
"…people who work with models always tend to overestimate their models, They come to believe models are real and forget they are only models." —polymath Freeman Dyson www.nytimes.com
Unfortunately there's a lot more to this than just over-confidence in computer models.
First and possibly most egregious—there are so many "egregious" it's hard to rank them—is the way the political/bureaucratic/pseudo-scientific/newsie Blob steadfastly confuses "infections" with "cases." Like this for example—
The United States marked a record number of coronavirus cases Friday for the third consecutive day, notching 77,638 new infections in 24 hours, according to a tally by Johns Hopkins University. —US sets another virus record with 77,638 new cases: Johns Hopkins
So, are they cases or are they infections? In the real scientific world, things simply aren't done that way. In his letter to German Chancellor Angela Merkel , thoroughly credentialled virologest Dr. Sucharit Bhakdi put it like this—
"In infectiology—founded by Robert Koch himself—a traditional distinction is made between infection and disease. An illness requires a clinical manifestation. [1] Therefore, only patients with symptoms such as fever or cough should be included in the statistics as new cases. In other words, a new infection—as measured by the COVID-19 test—does not necessarily mean that we are dealing with a newly ill patient who needs a hospital bed."
Bottom Line: A case reqires an infection but an infection is not a case.
With any disease—seasonal flu for example—there are always infected folks with mild or no recognized symptoms who don't enter the medical system. They're called "asymptomatic" but the newsies etc. pretend it's new with COVID-19 and scary.
But to heck with the newsies, keeping in mind that infections are not cases, let's see if the politicians and health bureaucrats stick to Koch's basic science—
In a Commissioners Court hearing for Collin County [Texas] on May 18th, it was revealed that while previously the determination of a Covid "case" was a confirmed test result , the definition was suddenly changed to count "probable" cases as "cases." … Even worse, once a "probable" case was determined based on possibly unrelated subjective criteria, up to 15 people in possible contact with that "probable" case were also listed as "probable cases." And " probable cases" were considered cases. … Is the Texas Covid 'Spike' Fake News?, By Ron Paul [bolding emphasis added]
So, by calling "confirmed test results" —which only indicates an infection—"cases," even before The Blob gets out the gate it's already completely off the infectiology reservation. Worse according to The Blob—and now flying in the face of Koch's scientific baseline at MACH 2—apparently if you say hello in person to someone who was probably infected, you're automatically escalated right through "infected," and directly into a "case" yourself as are up to 14 other friendly folks.
So even POSSIBLE infections have been escalated into full-blown "cases ." The more testing, the more infections you'll find—but you call them "cases" too. So if you're wondering where all these "spikes" are coming from, now you know. They're being mostly defined and imagined into existence.
To paraphrase Stalin, "It's not the infections, cases and deaths that define the 'pandemic,' it's those who report the infections, cases and deaths."
So now we know the official "cases" statistics, whether generated by tally or computer, are technical fiction and/or pretty much garbage.
So, unless you want to be completely misinformed, you can just about completely disregard official figures and stats so far—and those who purvey them.
Unfortunately the source of this unscientific and basically dishonest reporting goes much deeper than just " probable cases" in Collin County, Texas. It also includes reported deaths.
For example—
The city [New York] has added more than 3,700 additional people who were presumed to have died of the coronavirus but had never tested positive. —N.Y.C. Death Toll Soars Past 10,000 in Revised Virus Count - The New York Times [emphasis added]
Notice the word "presumed"—and " never tested positive" in the above. So the official stats admittedly include presumed coronavirus deaths as well as Collin Co's "probable cases." That "3,700 additional people" amounted to more than a 50% increase in reported NYC COVID-19 deaths at the time—all of them "confirmed" and/or "verified" by presumption.
And, if it can be done by presumption, what exactly do "confirmed" and/or "verified" actually mean?
Further, keeping in mind that among many other mislabeled causes of death as you'll see, until May 26, 2020, the C.D.C.s list of symptoms for recognizing COVID-19—and those for recognizing seasonal influenza —are almost identical. How could they tell the difference? So, how good were those presumptions anyway?
So, not only are the official "case" stats pretty much garbage, so are the official death stats. How much is "pretty much?" Stay tuned.
While this makes for exciting reportage and attention-getting politics, clearly it isn't science and it isn't correct.
So, "Why would Collin Co. Texas, New York City, etc. do that?" you ask?
From that same Times article—
The C.D.C., in its guidance to local governments, has recommended that cases of "assumed" coronavirus infection be noted on death certificates since before New York City recorded its first death on March 14. [bolding emphasis added]
So, they would do that because the C.D.C. recommended that they do. Why would the C.D.C. recommend something that seriously unscientific and misleading—and do it even before any deaths?
That's a very interesting question you may want to keep in mind while deciding, "Truth, Conspiracy or SNAFU."
And, in case there's any doubt U.S. Government health institutions—following C.D.C.s guidelines—did indeed recommend padding the figures with "probable infections" and " 'assumed' infection[s]" listed as "cases"—and presumed COVID-19 deaths without proof—
Dr. Scott Jensen, a Minnesota physician and Republican state senator said he received a 7-page document coaching him to fill out death certificates with a COVID-19 diagnosis without a lab test to confirm the patient actually had the virus. —MN Senator and Dr. Reveals HHS Document Coached Him on How to Overcount COVID-19 Cases
… and this from Trump-team star Dr. Deborah Birx—
"We've taken a very liberal approach to mortality. "…"If someone dies with COVID-19, we are counting that as a COVID-19 death," Birx said. —Dr. Birx Confirms Anyone Who Dies WITH Coronavirus, Regardless of Any Underlying Health Condition, is Being Counted as a COVID-19 Death
Also note (directly below) how the Italian health system—where the reported fatality rate and death toll were used to warn—OK, scare—everyone, similarly fudged the Italian COVID-19 numbers—
"The way in which we code deaths in our country is very generous in the sense that all the people who die in hospitals with the coronavirus are deemed to be dying of the coronavirus." —Professor Walter Ricciardi, scientific adviser to Italy's minister of health, telegraph.co.uk
Particularly note the similar language used by both Dr. Birx and Prof. Ricciardi—"very liberal approach to mortality " (Dr. Birx) and "very generous" (Prof. Ricciardi). Such very similar language implies a common source. Is there one?
And just how "very liberal" and " very generous" are those mortality numbers? And how scientific?
Before answering those questions, let's nail-down the common source where this misleading and unscientific reporting practice actually originated. I stumbled on the final troubling nail buried in this Bloomberg article—
As Russia's surging coronavirus infections have turned it into a global epidemic hotspot second only to the U.S., one thing puzzles health experts: Why is it reporting so few deaths? —Experts Question Russian Data on Covid-19 Death Toll - Bloomberg
Notice the typical anti-russia slant . But it's what comes next that nails the common source we've been looking for—
The Geneva-based agency of the United Nations (W.H.O.) issued guidelines in mid-April asking countries to register fatalities linked to Covid-19 "where the disease caused, or is assumed to have caused, or contributed to death." …. The mortality rate is low in Russia because the statistics only include the deaths of people directly attributed to Covid-19, said an official with knowledge of coronavirus fatality calculations. Other countries with higher totals have broader criteria for attributing deaths to the virus. More than 60% of fatalities of people suspected of having contracted Covid-19 [in Russia] are not classified as coronavirus deaths because they occurred "from clearly other causes," the Moscow health department said in a statement on its website, noting that autopsies are performed in all suspected cases. … Experts Question Russian Data on Covid-19 Death Toll - Bloomberg [bolding added]
So, it seems, both C.D.C. and W.H.O. are the common source of the misleading and anti-scientific reporting. And our first estimate of how "very liberal" and how "very generous" is that " more than 60%" of Russians suspected of dying of COVID-19 didn't. They died "from clearly other causes. "
And W.H.O. and the world health establishment join the C.D.C. in violating basic infectiology science—and then they all diss Russia for telling the truth.
So, instead of questioning Russia's solid science-based death toll, why didn't the experts question the grotesquely " more than 60% " inflated and scientifically indefensible death toll created by following the instructions from C.D.C. and W.H.O.? What IS going on here?
Why would W.H.O., C.D.C., etc. do that? Hard to tell for sure, but this is interesting—
"The FDA receives 45% of its annual budget from the pharmaceutical industry. The World Health Organization (WHO) gets roughly half its budget from private sources, including Pharma and its allied foundations. And the CDC, frankly, is a vaccine company; it owns 56 vaccine patents and buys and distributes $4.6 billion in vaccines annually through the Vaccines for Children program, which is over 40% of its total budget." - Robert F. Kennedy, Jr… [source]
and this—
The corporate takeover of W.H.O. youtube
And, since the establishment hasn't been honest, there are conspiracy theories of course—
The Farce and Diabolical Agenda of A "Universal Lockdown", By Peter Koenig, Global Research
The Covid Set-Up Is Now Fully in Play as CDC Outlines Plan for Death
For whatever reason they do it, I think we can safely say that what passes for the world health establishment is clearly all-in padding and distorting the official COVID-19 stats and figures into something that would even embarrass "fake news."
So help me out here. What do you think at this point? Is the official COVID-19 narrative true, a conspiracy, or just another SNAFU ?
But now, with padding and distorting in mind—and knowing where that came from—we're prepared to answer, "Just how ' very liberal' (Dr. Birx) and 'very generous' (Prof. Ricciardi) not to mention 'how padded and distorted' are those Stalinesque world health establishment mandated COVID-19 death numbers?
We already know they included about a third of those originally reported early deaths in NYC—unscientifically presumed to be caused by COVID-19 without tests.
But OK, ignoring some of the problems with the tests for now, what could possibly be wrong with the reported figures when tests have been used?
Although it's not immediately obvious, we already know. As the CDC requested—and Dr. Birx and Prof. Ricciardi verified—" If someone dies with COVID-19, we are counting that as a COVID-19 death…"
So, what's wrong with that?
"…the mistake is being made worldwide to report virus-related deaths as soon as it is established that the virus was present at the time of death—regardless of other factors. This violates a basic principle of infectiology: only when it is certain that an agent has played a significant role in the disease or death may [that] diagnosis be made. " —ibid, infectiologist Dr. Sucharit Bhakdi
The difference between dying FROM COVID-19 versus dying WITH COVID-19 may seem trivial but, in practice and by science—originally established by seminal infectologist Koch himself remember—it's extemely important.
Suppose for example, Uncle Joe checked into a hospital with a mild concussion from falling while suffering a stroke. Would they treat the concussion or the stroke? If Uncle Joe dies, was it the mild concussion that killed him or the stroke? Which would you list on the death certificate?
The same goes if you check into a hospital with a COVID-19 infection and pneumonia. That is, if you really did have a COVID-19 infection.
The concussion and COVID-19 are called co-morbidities—and/or pre-morbidities—and which one caused death is obviously a critical determination, not only for treatment, but also for accurate analysis.
Here's a real-life example—
"There was a report in Orlando a week or so ago, where you had someone in a motorcycle accident [die], unfortunately," the governor recalled. He said the motorcyclist's death was categorized as one of the 5,500 reported in relation to the novel coronavirus outbreak in Florida, "just because the person had previously tested positive." —Florida Gov. DeSantis Suggests COVID Death Toll Is Inflated
I have a friend whose 95-year-old mother was hospitalized for COVID. On day two of the hospitalization, the patient died of a massive heart attack. Guess what the primary cause of death was listed on the death certificate? If you guessed COVID-19, you win the prize…. Because of this, COVID will be diagnosed as the cause of death far more than it should. —Dr Brownstein | Fake COVID-19 Death Numbers [As you can see, The Federal Trade Commission coerced Dr. Brownstein into taking that page down .]
So we have "infections" illegitimately called "cases"—and now, deaths attributed to the virus simply beause it may have been present.
But you want numbers, right?
We already know that "more than 60%" of suspected Russian COVID-19 deaths were from "clearly other causes," and not from COVID-19 but we can do better.
As reported by Bloomberg, based on a study by Italy's official Istituto Superiore Di Santita , when Italy began to re-evaluate and report their results without fudging the supposed COVID-19 caused fatalities they found—
…just three victims, or 0.8% of the total, had no previous pathology. Almost half of the victims suffered from at least three prior illnesses and about a fourth had either one or two previous conditions. More than 75% had high blood pressure, about 35% had diabetes and a third suffered from heart disease. [that is, 99.2% suffered at least one pre-morbidity] —99% of Those Who Died From Virus Had Other Illness, Italy Says - Bloomberg
Prof. Ricciardi sums it up like this—
"On re-evaluation by the [Italian] National Institute of Health, only 12 per cent of death certificates have shown a direct causality from coronavirus, while 88 per cent of patients who have died have at least one pre-morbidity - many had two or three," [Professor Ricciardi] says. telegraph.co.uk
So only 12% of Italian deaths can be directly attributed to COVID-19. Co-morbidities—that is, "clearly other causes"—killed the other 88%.
And then there's this rather embarrassing revelation—
"Had the CDC used its industry standard, Medical Examiners' and Coroners' Handbook on Death Registration and Fetal Death Reporting Revision 2003, as it has for all other causes of death for the last 17 years, the COVID-19 fatality count would be approximately 90.2% lower than it currently is." [source] and a tip-o-the-hat to Jon Rappaport
So, by sneaking deaths caused by co-morbidities into their guidelines, the world health establishment managed to inflate COVID-19 deaths by more than eight times!
What do you suppose they'd find if they honestly re-examined U.S. death certificates?
It's reasonable to suggest that in the country that followed CDC guidelines which "recommended that cases of 'assumed' coronavirus infection be noted on death certificates since before New York City recorded its first death on March 14,"—and, as directed by the CDC itself, ignored the CDC's own guidelines—that they would find a similar 12% COVID-19 to 88% co-morbidities ratio. Let's go with that.
As a result, you get the next "egregious "—you get the "official stats" for case fatality rate as elegantly displayed by the gonzo Johns-Hopkins/arcgis.com COVID-19 app showing " Confirmed Cases " and " Global Deaths ."
Definitely an elegant app but we know the figures aren't even close because they include infections as "Confirmed Cases" and about 88% of the "Global Deaths" can't legitimately be attributed to COVID-19.
Garbage in, garbage out.
Worse yet, even if the numbers were accurate they produce a seriously misleading fatality rate—called the "case fatality rate." The "case fatality rate" measures how many of the sickest folks, that is, the folks who come to the attention of the medical system die, most in care homes and hospitals.
For example, on June 3, 2020, 10:03:14, the Johns-Hopkins numbers showed that for every 17 folks who came to the attention of the medical establishment, one of them died for a case fatality rate of about six percent (6% ). We now know that's garbage to start with because approximately 88% of them died from co-morbidities, not from COVID-19.
And remember "most [die ]in care homes and hospitals" for later.
But what about all those "asymptomatic" folks who don't come to the attention of the medical system?
They're important because, rather than the scare-number of how many folks with serious symptoms and pre-morbidities die, we want to know "How many of the folks infected with COVID-19—including all those "asymptomatic" folks—die from COVID-19?" That is, we want to know the "infection fatality rate ."
To figure that out, we need to know how many folks in a whole population are infected, not just the sick ones that enter the medical system. That's a much larger number of folks—many who are "asymptomatic" remember—and we don't know who or where they are, which makes this a much harder question to answer. It requires statistics and careful sampling—
One of the first studies —Santa Clara Co. California—conducted by 17 researchers including Prof. John P.A. Ioannidis , who, commenting on the lack of evidence for the extent of infections , pointed out in early March that —
This evidence fiasco creates tremendous uncertainty about the risk of dying from Covid-19. Reported case fatality rates , like the official 3.4% rate from the World Health Organization [WHO], cause horror - and are meaningless.
Note that the flawed Johns-Hopkins numbers he's referring to already implied a much higher 6% case fatality rate on June 3.
With scientific humility, often missing these days, Prof. Ioannidis describes the results of that Santa Clara study like this—
"…the number of infected people is somewhere between 50 and 85 times more …compared to what had been documented [as cases]. Immediately that means the infection fatality rate, the chance of dying, the probability of dying if you are infected diminishes by 50 to 85 fold…. Our data suggests that COVID-19 has an infection fatality rate that is in the same ball park as seasonal influenza. " [emphasis added]
You can find extensive results from other subsequent similar studies—verifying COVID-19's infection fatality rate is about the same as seasonal influenza—collected here.
So why don't "we" mandate what are essentially ceremonial masks , social distancing and other symbolic measures that have little effect—and of course, lock-down the world economy—to try to stop seasonal influenza every year?
But these studies only calculate the infections—they accept the official death tally at face value. Let me repeat that: They accept the official death tally at face value.
That means these studies are assuming those 8x inflated C.D.C.-W.H.O. death-toll numbers are correct. That means the actual caused-by-COVID-19 infection fatality rate is only about 12% of what these studies suggest. In other words, COVID-19 is only about 12% as serious as the seasonal flu—and 88% less dangerous!!
Putting numbers to it, as of July 30, 2020, the 7x inflated Johns-Hopkins numbers claimed 150,713 U.S. COVID-19 deaths. Instead, applying the 12% correction, there were actually only about 18,085. Clearly the officially reported—and so-called verified and/or confirmed—COVID-19 deaths and cases are complete fiction that would even make Stalin wink.
So it's completely clear, it's not the virus pandemic we have to worry about, it's the Narrative Pandemic .
Still, while the statistical truism that " correlation does not imply causation" obviously applies, if COVID-19 isn't responsible, why does it keep mysteriously showing up correlated with all these co-morbidities, cases and deaths?
The biggest and most obvious part of the answer is that the C.D.C.-W.H.O. guidelines specifically instructed the world-wide medical establishment to illegitimately create that correlation with incorrect and misleading record keeping and reporting. And in some cases, gave cash incentives for doing it.
In fact, as John Rappoport hypothesizes, there's an outside possibility that the dangers of COVID-19 may be mostly a statistical artifact produced by the fake statistics connecting it to the real killers, the co-morbidities.
Why would the world-wide elitist establishment do that?
Well, to give them at least a limited-hang-out excuse, they might claim they were afraid "we" wouldn't take their warnings seriously if they didn't wildly exaggerate things.
On the other hand, there's the suggestion that this was their answer—for those willing to kill hundreds of millions, mostly by starvation —to perceived over-population and CO ˛ emissions.
And of course, there's always SNAFU—
But still, "People are dying!" In fact, more people are dying than would be dying without the COVID-19 scare. Why?
There are two other "co-morbidities" that are rarely recognized and almost never mentioned because it's more convenient—and "politick"—to blame them on COVID-19.
The first is "politician." No, I'm not kidding.
Keep in mind that approximately half of all world-wide deaths blamed on COVID-19 happened in extended care facilities .
What's that have to do with "politician" as a co-morbidity?
See, New York governor Cuomo insisted on putting known COVID-19 patients in personal care-homes amongst the vulnerable elderly. Like this:
[New York] Gov. Andrew M. Cuomo continued to defend his decision to place recovering COVID-19 patients into nursing homes, even though it brought him some “political heat,” he admitted on Sunday. Cuomo defends decision to put COVID-19 patients in nursing homes | Newsday
New Jersey governor Phil Murphy emulated Cuomo and Pennsylvania governor Tom Wolf did the same, leading to this question at one of Wolf's media events:
~"70% of COVID-19 fatalities in Pennsylvania are from nursing homes and personal care homes. What are your plans to deal with this?" —question to Rachel Levine, PA Sec. of Health, Chanel 4 news, Tuesday, May 12, 2020 2:24 PM,.
The same really stupid policy—unless it was intended to get rid of a lot of older folks who were draining government coffers—was encouraged by a Ł1,000 bounty in the UK and has been laid at BoJo's (Prime Minister Boris Johnson's) feet—
UK Council gave care homes Ł1000 as 'cash incentive' to take in Covid patients.
Hence "Politician" as a co-morbidity. Does this help explain the care-home death toll in the rest of the world too?
The second rarely mentioned co-morbidity is " hospital."
You enter a hospital with one malady but die from an in-hospital screw-up of some sort or a disease you get while there instead. That's called iatrogenic death. If it doesn't kill you, it's an iatrogenic illness.
Even before this COVID-19 fiasco, "…hospital was the third leading cause of death in the U.S."
In the previously referenced article—the one the FTC coerced him into taking down —Dr. Brownstein explained that " Hospitals receive …up to $13,000 from the Government for an admission diagnosis of COVID, " and " if the patient is ventilated, they receive up to $39,000. "
"I can guarantee you that hospital administrators are running around telling every physician and resident physician to diagnosis COVID at the first cough or sneeze," Dr. Brownstein suggests.
So, besides possibly treating folks for COVID-19 instead of for the co-morbidities they were there for, in addition—maybe to get the bounty—did they also hospitalize some who, fearing for their lives because of the narrative, wouldn't have otherwise been hospitalized? If so, this would needlessly expose them to " hospital."
Were there additional COVID-19-fiasco-related hospital screw-ups and deaths?
Here's a clue—
~"If you were ventilated at the beginning of the pandemic, you had an 80 or 90 percent chance of dying, now you have an 80% chance of recovering." —Dr. William Haseltine, President, Access Health International, Author "A Family Guide to Covid," Bloomberg, Tuesday, June 16, 2020 2:50 PM
Accepting Dr. Haseltine's numbers and doing the math, at the beginning of the "pandemic," at least eight of ten ventilated patients died when, by best practices later on, only two of ten died. That means that six of ten early-on ventilated patients didn't die of COVID-19—or whatever—they died because they were ventilated and/or incorrectly ventilated, classic cases of iatrogenic death.
How many death certificates do you suppose actually reported it that way?
And how many folks were put on ventilators, partially at least to collect that $39,000? Does that implicate "politician " as a co-morbibity again?
Further, instead of ventilation, "best practices " in large numbers of patients was actually a practice called "proning", much safer with better outcomes than ventilating but without the $39,000 and so far pracitced in only a few hospitals.
Factoring that oversight into the death figures would obviously increase the iatrogenic—and overall—"hospital" (as opposed to COVID-19) co-morbidity death toll. Maybe someone will eventually do the research and math to get a solid figure.
Were there still other political and medical system screw-ups that ended up with COVID-19 on the death certificate instead?
Three whistle-blowing nurses verify over-ventilation—and bring a few other troubling modern hospital issues to light here: Misconduct in NY hospitals—three nurses speak out!
Most troubling is the apparent consensus among those nurses that when you go into a hospital, "pandemic" or not, you should take an "advocate" with you.
"From my perspective as a physician (family practitioner) and from the perspectives of some other candid colleagues in medicine, nursing, dietary, et al, large numbers of deaths were simply due to institutional panic, malpractice and neglect." —S. Athanail MD, Brooklyn, NY
So care-home deaths due to politicians housing COVID-19 patients in them, unnecessary bounty-driven hospitalizations that ended in death, ventialting patients rather than proning them and ventilating patients outside of later-discovered best practices added to all those other co-morbidities reflexively blamed on the virus would all help explain the approximately 88% of deaths incorrectly blamed on COVID-19.
At any rate, you would expect these "hospital " and "politician" co-morbidities to decay out and the death-rate to decline as the politicians & hospitals correct themselves. Instead of "we wildly exaggerated," the excuse you hear to explain that exact effect, now happening all over the world is that "covid-19 is getting weaker"—
CDC quietly DOWNGRADED Covid-19 death rate and media IGNORED good news. Elon Musk wonders why
Cases are going up in Louisana but ICU admissions and deaths are flat. —Sen Bill Cassidy, Bloomberg, Thursday, July 09, 2020 12:47 PM
And now The Blob's problem is, once it becomes obvious that COVID-19 was wildly exaggerated, heads will roll or worse, so a lot of the world's top-tier establishment is desperate for more COVID and more horror stories. With about 7 billion humans on Earth, guaranteed they will find them. And, just like the number of COVID-19 cases and deaths, you can always just make them up too.
Here's one of the tricks, thanks to a tip from a credible source: Record each positive test as an infection. That means when a second or third etc. test is given to a patient to verify or track a positive, each positive test shows up in the records as a separate infection. So if one patient is given, say, 14 tests over a two-week period—which is common practice in tracking an infection—and they're all positive, that one patient shows up in the records as 14 separate infections. And of course, they're all reported as full-blown " cases." .
[Fla. Governor] DeSantis also … proposed a " testing-industrial complex" was responsible for the recent wave of Florida residents who say they received positive virus diagnoses without taking a test. —Florida Gov. DeSantis Suggests COVID Death Toll Is Inflated
Also once the COVID-19 meme was established, it evolved into an increasingly powerful self-reinforcing memetic statistical "attractor" and a much-needed eye-magnet for the newsies—and it became more and more popular as an excuse for disparate "bazarre symptoms" and circumstances that almost certainly have nothing at all to do with COVID-19.
Scientists identify six different types of coronavirus with increasing severity levels
The latest is "Experts say 'the second wave' may target the young. " I wouldn't doubt it for a second—IF, that is, you interpret that as, "' the second wave' of narrative nonsense may target the young. " It's pretty clear they're now trying to terrify the younger folks, many of whom have caught on to the scam.
Even their own worst fake figures—the 8x inflated CASE Mortality Rate for example—show that clearly youngers—if they even get infected—have almost nothing to fear, despite the scare-mongering narrative—
8x Inflated COVID-19 CASE Mortality Rate by Age
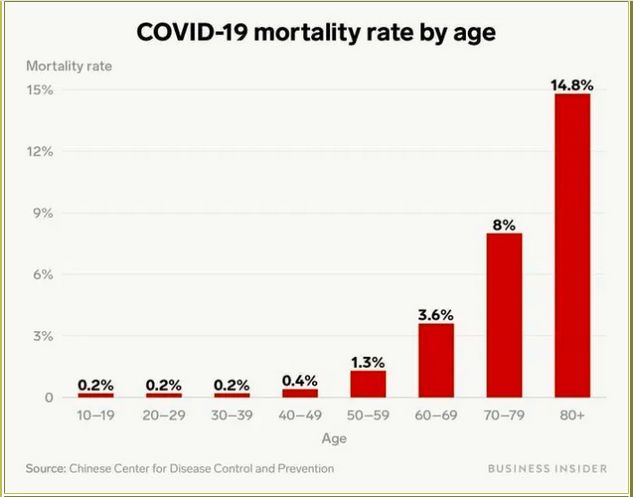
via Business Insider
So, will COVID-19 kill you? Will the economy re-open?
Clearly not until the COVID-19 Narrative Pandemic is cured.
But, with their own self-preservation in mind, can you imagine House Speaker Pelosi, Governors Cuomo, Wolf and Murphy, PM Boris Johnson etc. coming out of the COVID closet and telling us, "I'm sorry. We got it wrong. We wildly exaggerated COVID-19. We destroyed the world economy and impoverished and starved much of the population by mistake. "
So while COVID-19 is unlikely to kill you, the politicians, their economic ignorance—MMT for example—and the Narrative Pandemic might.
Even if you choose to believe the official figures, even if you're over 60 and/or have co-morbidities, it almost certainly won't kill you. Even if you're over 60, the odds are overwhelmingly in your favor. And that's IF you actually get infected. Assuming the official figures are accurate, it looks something like this—
Infection Fatality Rate by age (China)
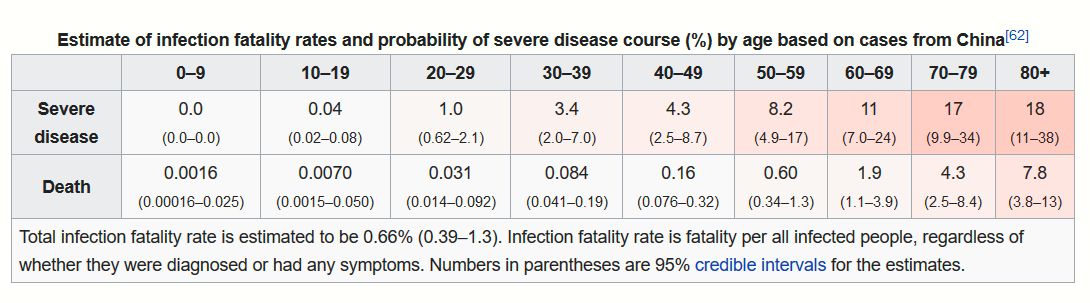
If you stay out of hospitals—and care homes —the odds are much better.
Since nearly all the deaths occur among those over 60, why should the youngers destroy their lives and the lives of the next several generations so we olders can walk around imagining we're safe and protected because folks are wearing what are essentially ceremonial masks ? Especially since they eliminate most of the 60%-plus of the non-verbal communication we humans count on so heavily.
And, so far, you don't have to . And if you run a business, there's this—
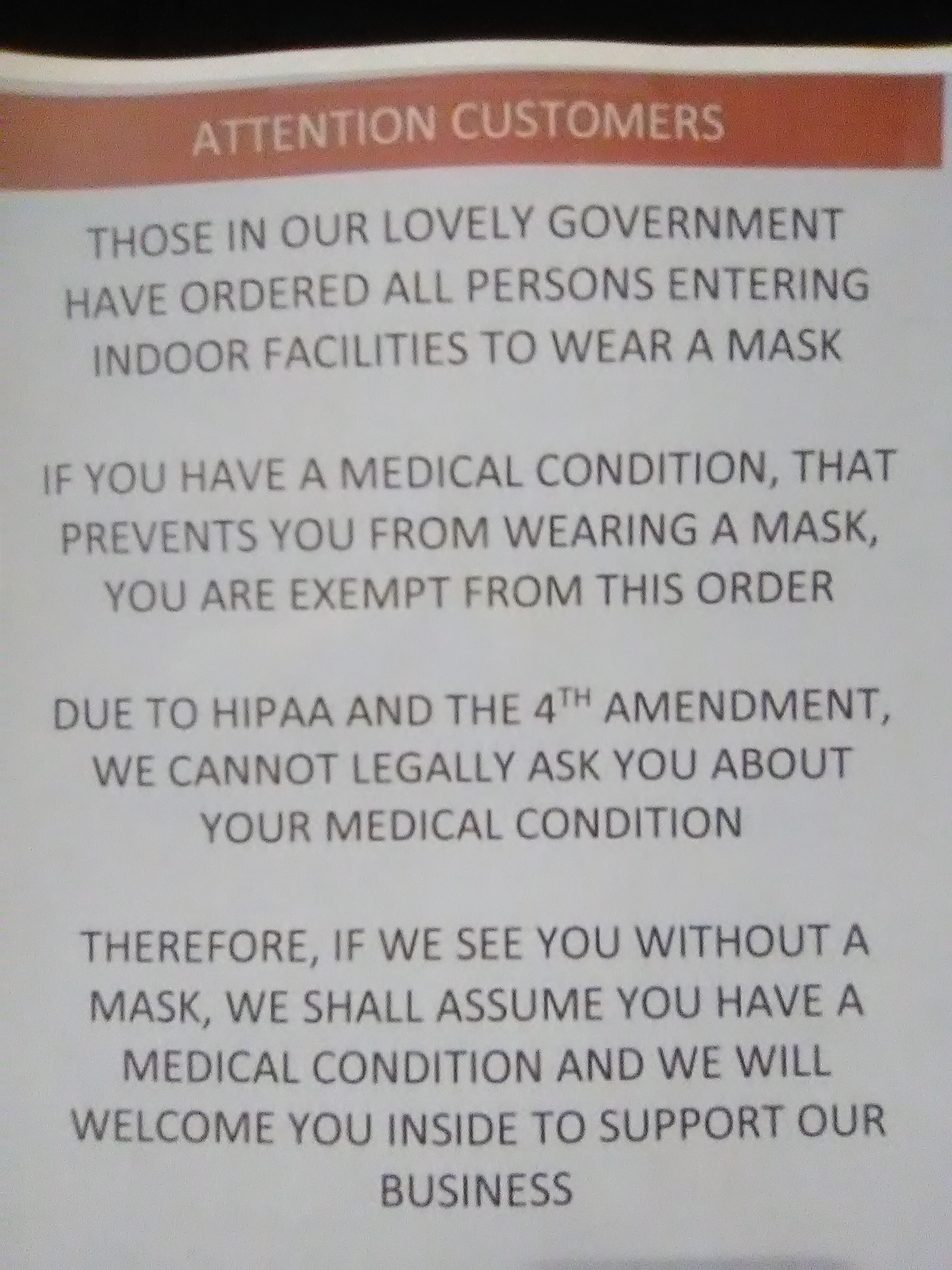
On the bright side, masks mess up facial recognition.
Even if the stats weren't fake news, "locking-down" the economy to save grandpa is like trying to shoot a gnat with an elephant gun—except you and grandpa are in a metal-walled room and the bullets ricochet.
BTW, the stock markets etc.—don't count this time. They aren't part of the real economy any more or even an indication of how it's doing.
They've become score-cards for how well the stock-and-bond gamblers, corporate financial engineers, and particularly the high-frequency-trade "algos" are doing with the free money and "back-stop" promises the Federal Reserve and other Central Banks are creating for them out of thin air. They're now completely creatures of super computers and Central-Bank-created Moral hazard .
And of course, the government won't admit it wildly screwed-up. Even if it did, most folks don't trust "our" elected fools, dupes, psychopaths and liars anyway, so rather than a "re-opening," the best we can hope for is a re-evolution.
If we can get That Thing That Lives in Washington D.C. —and in State Capitols—out of our way.
And, BTW, what do you think?
COVID-19: Truth, conspiracy, or SNAFU? Here for updates, additions, comments, and corrections.
AND, "Like," "Tweet," and otherwise, pass this along!
L. Reichard White [send him mail] taught physics, designed and built a house, ran for Nevada State Senate, served two terms on the Libertarian National Committee, managed a theater company, etc. For the next few decades, he supported his writing habit by beating casinos at their own games. His hobby, though, is explaining things he wishes someone had explained to him. You can find a few of his other explanations listed here .
ADDENDUM—
A thoughtful reader made this observation by email, however it was mostly the discovery in checking his included link that caused me to attach this addendum—
My question however, concerns the overall increase of deaths in 2020 as there have been considerably more deaths in 2019/2020 versus the same time periods in the previous four years.
The death numbers presented below were extracted from the July 26, 2020, data file titled 'National_2015-20_Data.csv' downloaded from https://gis.cdc.gov/grasp/fluview/mortality.html.
The average of all cause deaths according to the CDC for weeks 40 through 52 and 1 through 27 for the four years starting in 2015 and ending in 2019 was 2,180,841.
However, for weeks 40 through 52 and 1 through 27 in 2019—2020, all cause deaths exceeded the average of the prior four years by 188,560. —Greg Quick Mon, Aug 10 at 2:10 PM
Thanks for your excellent observation and link, Greg Q.!
However the page you linked above is now blocked by a "Disclaimer" that can't be removed, you can't see most of the page, and it is thus now unusable. AND that "Disclaimer " shows up in the WayBack archived versions as well. Here for example: National Center for Health Statistics Mortality Surveillance System
As of Aug. 11, 2020, it looks like this—
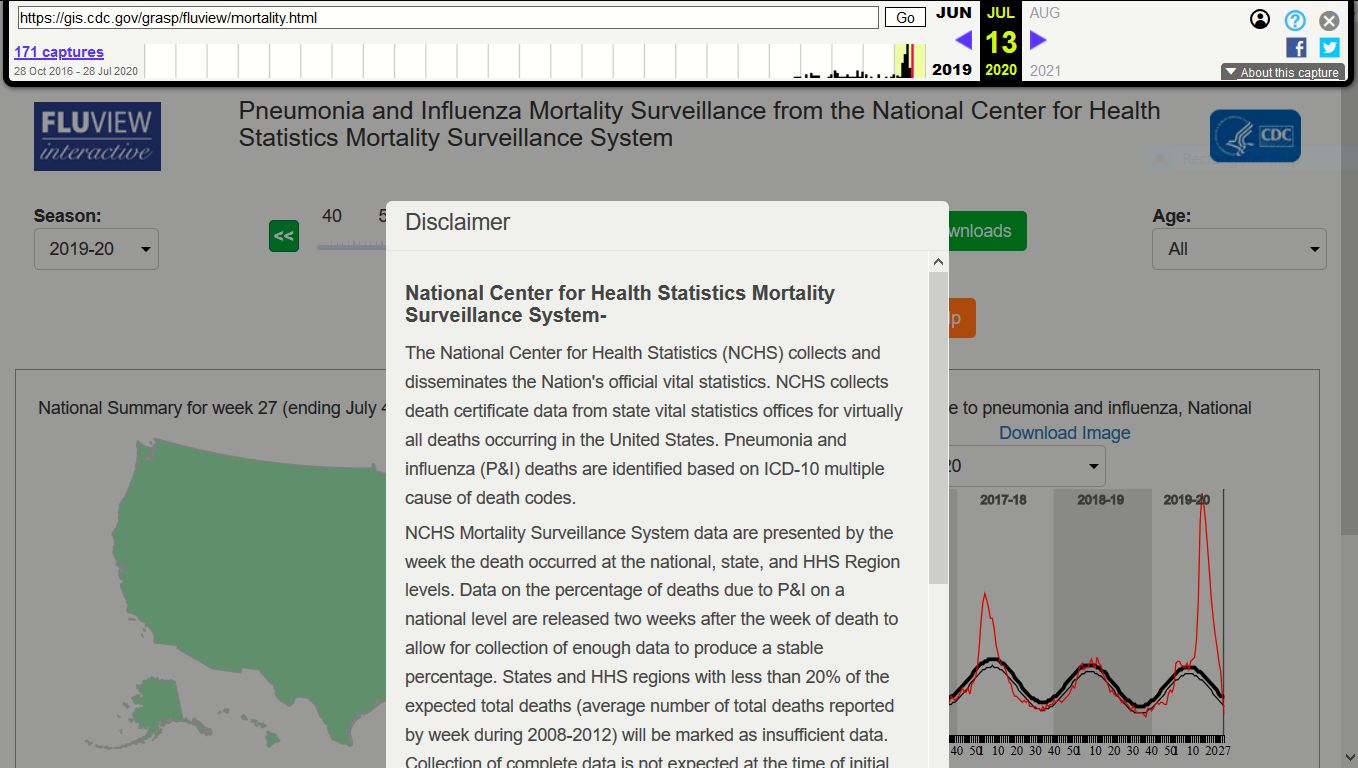
Regardless, your question dragged me back into the fray and the
result is below—
1. According to Italy, Russia and the CDC's own guidelines, only something like 12% of reported COVID-19 deaths were actually caused by COVID-19. That's the bottom line.
2. The sudden 2019-2020 blip up and back down is only about a 10% increase over average and significantly less compared to the 2017-2018 blip you can see right beside the "Disclaimer" blocking our view.
3. It's almost certain that official numbers they give us are, like the original scare numbers, computer generated—there's no way world-wide bureaucracies are nimble enough to keep up anywhere near real-time. My best guess: these numbers are like the electronic election projections only not able to be "instant breakfast" like election projections and returns.
4. Given the proven lack of honesty with the way the numbers have been generated in the first place—as layed out in " The Narrative Pandemic"—well, to paraphrase Stalin, " Infections, cases and deaths don't define the pandemic, those who count and report them define the pandemic."
5. Iatrogenic deaths likely played a part in the maybe 12% of reported deaths that may have actually been caused by COVID-19—
"From my perspective as a physician (family practitioner) and from the perspectives of some other candid colleagues in medicine, nursing, dietary, et al, large numbers of deaths were simply due to institutional panic, malpractice and neglect." —S. Athanail MD, Brooklyn, NY
6. And again, the bottom line is that only something like 12% of the asserted COVID-19 deaths—at most—may actually be caused by COVID-19.
lrw.
It's About Those Official Corona Virus Figures … No, this isn't a conspiracy theory—March 14, 2020
The Rock vs. the Hard Place, COVID-19 vs. The Economy, April 12, 2020
Truth, Conspiracy, or SNAFU -You Decide, July 25-26, 2020
—My COVID-19 Interview with David Forsyth of "Your Freedom Adventure"
Was that worth reading?
Then why not:
![]()
|
Support this online magazine with
|
AFFILIATE/ADVERTISEMENT
This site may receive compensation if a product is purchased
through one of our partner or affiliate referral links. You
already know that, of course, but this is part of the FTC Disclosure
Policy
found here.
(Warning: this is a 2,359,896-byte 53-page PDF file!)
L. Neil Smith‘s The Libertarian Enterprise does not collect,
use, or process any personal data. Our affiliate partners,
have their own policies which you can find out from their websites.
