Is it COVID or Is it the Flu? Not Even Your Doctor Knows for Sure.
by L. Reichard White
[email protected]
![]()
Special to L. Neil Smith’s The Libertarian Enterprise
Either the COVID-19 pandemic is a SNAFU of truly cosmic proportions or it's a conspiracy—or, possibly, a little of both. Yes, there really are conspiracies of truly cosmic proportions.
SNAFU, conspiracy, or a little of both? I'm just here to help you decide.
Given the circumstances, I'm sorry to say, paraphrasing Joseph Stalin is the key to understanding this quite amazing event, like this—"It's not the infections, cases and deaths which define the 'pandemic,' it's those who count and report the infections, cases and deaths."
In part, this is because the numbers they're feeding us are almost exclusively computer-generated and so require programming assumptions. Unfortunately, that's not the only problem-
Your doctor normally has a very good idea what to treat you for from your symptoms. He then backs up his diagnosis with tests. But diagnosing COVID-19 based on your symptoms presents your doc with a very serious problem as the chart below, taken directly from C.D.C. [Centers for Disease Control] pages, demonstrates-
As you can see, except for "loss of taste or smell ," the symptoms of COVID-19 and the symptoms of Seasonal Influenza are identical. In fact as the chart shows, until May 26, 2020—that is for the first three months of the "pandemic" when there were almost no tests available—the symptoms were identical .
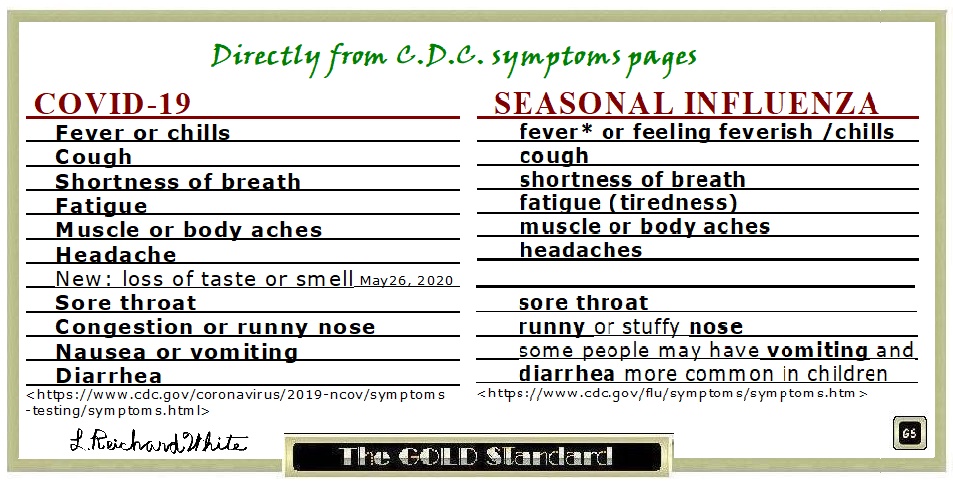
It's worth noting that on May 26, 2020, CDC officially added "New: loss of taste or smell." Maybe you remember?
There are two reasons that's note-worthy. First it's a symptom of zinc deficiency which weakens your immune response. Second when you have a stuffy nose, you automatically lose smell, and, strangely enough, taste heavily depends on smell so you lose that too.
You can verify this for yourself. Hold your nose, have someone blindfold you, and see if you can taste the difference between a bite of apple and then a bite of onion.
Clearly, with congestion and stuffy nose as symptoms, loss of taste and/or smell would apply to Seasonal Flu as well as to COVID-19. Surely C.D.C. knows that, right? At any rate, for all intents and purposes, the symptoms of both COVID-19 and Seasonal Flu are still the same.
So, without tests, what's a poor doctor supposed to do?
Well, the C.D.C. told your doctor what to do in early March, 2020, like this:
The C.D.C., in its guidance to local governments, has recommended that cases of "assumed" coronavirus infection be noted on death certificates since before New York City recorded its first death on March 14. [bolding added] —N.Y.C. Death Toll Soars Past 10,000 in Revised Virus Count - The New York Times
Before the first death? Really? And the Death Toll Soared—as the above NYT headline trumpets—because, following C.D.C. guidance, they lump-sum added 3,700 "presumed" COVID-19 deaths.
Just to make things clear,
Dr. Scott Jensen, a Minnesota physician and Republican state senator said he received a 7-page document coaching him to fill out death certificates with a COVID-19 diagnosis without a lab test to confirm the patient actually had the virus. —MN Senator and Dr. Reveals HHS Document Coached Him on How to Overcount COVID-19 Cases
This C.D.C. directive completely violates over 100 years of established and traditional scientific practice and the C.D.C.'s own Medical Examiners' and Coroners' Handbook as well.
So what happened as a result of C.D.C.'s aberrant directive?
In addition to instantly adding those 3,700 presumed COVID-19 deaths in NYC alone, by including COVID-19 so-called " related " deaths, it inflated the number of disingenuously asserted and reported COVID-19 deaths by a factor of 10
The results of this aberrant directive was almost certainly compounded by the up to $13,000 bounty the Federal Health Bureaucracy awarded hospitals for each COVID-19 admission.
So, given the identical symptoms of the flu to COVID-19, consider that despite C.D.C.'s estimate of 24,000 to 62,000 influenza deaths-
There have been fewer influenza cases in the United States this flu season than in any on record. About 2,000 cases have been recorded since late September, according to data from the Centers for Disease Control and Prevention. In recent years, the average number of cases over the same period was about 206,000…. —The Flu Vanished During Covid. What Will Its Return Look Like? New York Times
That's 2,000 current influenza cases compared to a normal average of 206,000 cases.
How many of those do you suppose were mis-diagnoses, mistaking the flu for COVID-19 because C.D.C. said to record them that way, the symptoms are identical, and because of the bounty?
And the flu didn't seem to disappear only in the United States—
Flu Has Disappeared Worldwide during the COVID Pandemic —Scientific American
Ok, but once the tests were available, the doctors could easily tell the difference, right?
Unfortunately, the tests and the ways they were used made things worse. Here's why—
Once you begin to think about dis-eases, there's an almost always neglected context—we are not alone in our bodies. We're accompanied by an incredibly large array of microorganisms. In fact, current estimates suggest that the number of those companions significantly exceed the number of our own cells .
For the most part, we coexist peacefully and even aid each other. The microfauna in our lower intestinal tract are necessary for digestion for example. It's to tune them up that some folks take those probiotic supplements.
Clearly we can't get rid of these little guys.
The thing is, when some of that overwhelming host of fellow travelers get out of line—or we're invaded by undesirable migrants—our millions-of-years-old immune system automatically takes care of things and we usually don't even notice.
In fact, some of the undesirable migrants are always around. This was just verified again in what would be a disturbing discovery if we didn't understand that our veteran immune system regularly keeps things under control.
A current reminder was the discovery, verified by the University of Florida , that some childrens' COVID masks had trapped some rather nasty migrants. For example, organisms that can cause tuberculosis, Legionaires disease, peneumonia, meningitis, peridontal disease, strep throat, acne, and many others.
The good news is that none of the children had symptoms of any of these diseases. Although they were infected, they were "asymptomatic," that is, showed no symptoms.
In fact, most of us are chronically, 24/7, infected with some of these bad boys but our veteran immune system is also on duty 24/7 and so we rarely notice. That's as it must be or the human race wouldn't have survived.
So when discussing any dis-ease, the question isn't " Do you have dis-ease organisms in your body?"—you certainly do—but "Are there enough of these organisms, alive, well and strong enough to overcome your immune system, and cause symptoms, and can you pass enough of them on to infect others?"
With that in mind, let's take a look at the test almost exclusively being used to detect COVID-19, that is, the PCR test.
Dr. Kerry Mullis—who won the Nobel Prize for developing the PCR—said it's too sensitive, especially when run at high amplification cycles, to be used to make primary diagnoses. None the less, that's the way it's usually being used.
An amplification cycle is sort of like doubling the magnification of a picture on your device and then doubling the resultant magnified image again and again and again etc.
The C.D.C. and W.H.O. told folks to run the tests as high as 45 amplification cycles and later, 35 cycles, both extremely high. The problem is that a sample that tests positive for an organism above 25 amplification cycles can't be cultured. That is, the virus, if it actually exists in that sample, can't be coaxed to reproduce, even in favorable laboratory conditions.
And of course, if those bad boys try to infect us, they have our veteran immune system to contend with.
The logical conclusion is if the virus can't even be cultured in favorable laboratory conditions, it won't be able to reproduce in the hostile environment of the human body and clearly can't be meaningfully transmitted.
In fact, that argument found its way into a French Court, correctly asserting that if the PCR test was to be used as an excuse for lockdowns—which have been proven ineffective in most circumstances (Peru, with the world's strictest lockdown and world's highest death rate is a good example) and often terminally damaging to large swaths of the world economy —the tests should be required to run at no more than 27 amplification cycles.
Since the PCR tests are still typically run well above 25 cycles, you get all those asymptomatic folks, testing positive for "infections" but who are not infectious.
If we were to take the greater than 25 PCR cycles results seriously – and tested for tuberculosis, Legionaire's disease, meningitis, etc., we'd all be confined to our own hermetically sealed bubble for life.
To compound the disinformation, such asymptomatic " infections" are almost always called "cases" by nearly everyone— dishonestly implying hospitalization . This dishonesty is especially egregious and troubling as it's displayed by the ubiquitous misleading Johns-Hopkins Bloomberg "WORLD SICK MAP" among others.
On the other hand, Florida Governor DeSantis required lower cycles in Florida's COVID-19 PCR tests and, surprise, suddenly the reported infections, "cases" and COVID-19 deaths there subsided.
Keep in mind while the PCR test may be used to verify a diagnosis based on symptoms, because of it's excess sensitivity, especially at high cycles, it identifies sub-clinical infections, which makes it a serious mistake to use it to make primary diagnoses.
None the less, when the bureaucrats mandate wide-area blind geographical testing, which is what most testing is—or scared folks with no symptoms show up to be tested—that serious mistake is exactly what they're making.
To compound the problem, on June 13, 2020, some element in the C.D.C. , which surely knew better, mandated that all patients that needed hospitalization for any reason be tested for COVID-19 at time of admission regardless of symptoms, and if tested positive, be logged as a COVID-19 patient.
And there's the up to $13,000 bounty.
As a result, someone who gets admitted to a hospital with, say, a broken bone may find themselves diagnosed and treated for COVID-19—whether they need it or not . And, should they die of complications, COVID-19 would likely be what was on the death certificate—and what was reported by the Johns-Hopkins Bloomberg " WORLD SICK MAP ."
So, given this SNAFU, conspiracy or a little of both—and keeping Stalin's paraphrase in mind—
Is it Really COVID at all?
Until they get the testing, reporting—and diagnosing—straightened out, Not Even Your Doctor Knows for Sure . Maybe you only have just that broken bone.
ADDENDUM: Establishment fast-talker, former FDA Commissioner, and admitted Pfizer board member Dr. Scott Gottlieb was doing the rounds last Sunday (June 27), standing on the " fear pedal" as hard as he could, conjuing-up the "delta variant panic porn" as some call it. Etc.
Unsurprisingly, since Pfizer has an experimental vaccine in the game, he was pimping vaccines, the new mRNA ones a bad bet for everyone , and for kids (who don't need them ), for younger adults—only a few will be affected—and warned everyone about " long COVID. "
Thing is, along with the other panic porn, the same "long" danger is nothing new—
"I can't find a single thing that the SARS-CoV-2 virus can do, that other viruses cannot," [microbiologist Amy] Proal said. "It's well understood and it's been understood for decades that every major pathogen capable of infecting people has a syndrome associated with it in which a certain number of patients who get that pathogen," she continued, "will develop chronic symptoms that never go away." … Long-term Covid-19 side effects aren't unique. H1N1, Zika, and strep throat also have chronic symptoms. - Vox
HERE for updates, additions, comments, and corrections.
AND, "Like," "Tweet," and otherwise, pass this along!
L. Reichard White [send him mail] taught physics and the Philosophy of Science, designed and built a house, ran for Nevada State Senate, served two terms on the Libertarian National Committee, managed a theater company, etc. For the next few decades, he supported his writing habit by beating casinos at their own games. His hobby, though, is explaining things he wishes someone had explained to him . You can find a few of his other explanations listed here .
Was that worth reading?
Then why not:
![]()
|
Support this online magazine with
|
AFFILIATE/ADVERTISEMENT
This site may receive compensation if a product is purchased
through one of our partner or affiliate referral links. You
already know that, of course, but this is part of the FTC Disclosure
Policy
found here.
(Warning: this is a 2,359,896-byte 53-page PDF file!)<
L. Neil Smith‘s The Libertarian Enterprise does not collect,
use, or process any personal data. Our affiliate partners,
have their own policies which you can find out from their websites.
